|
|
 |
 HOME > 증 례 003 HOME > 증 례 003 |
|
This sixty-eight-year-old woman was admitted with paraplegia. She could neither walk nor stand alone. The onset was insidious and weakness of both lower extremities had aggravated gradually since four months prior to admission.
The muscle power grades of the lower extremities were between three and four, and sensory changes were noted below the T6 level. The knee and ankle jerks were hyperactive, and unsustained ankle clonus was noted on both sides.
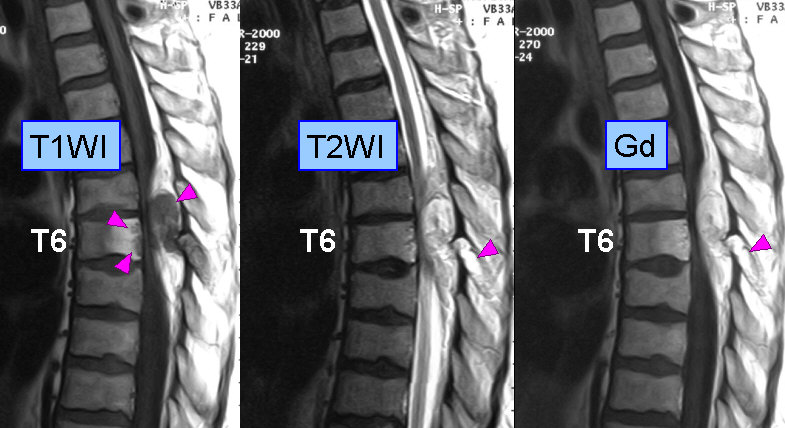
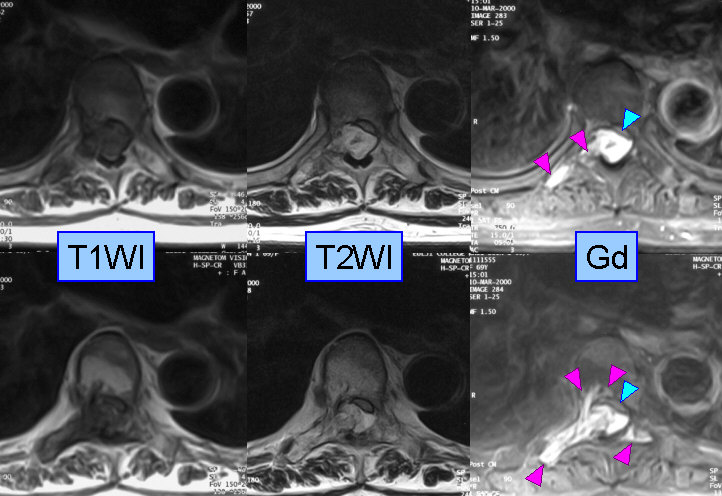
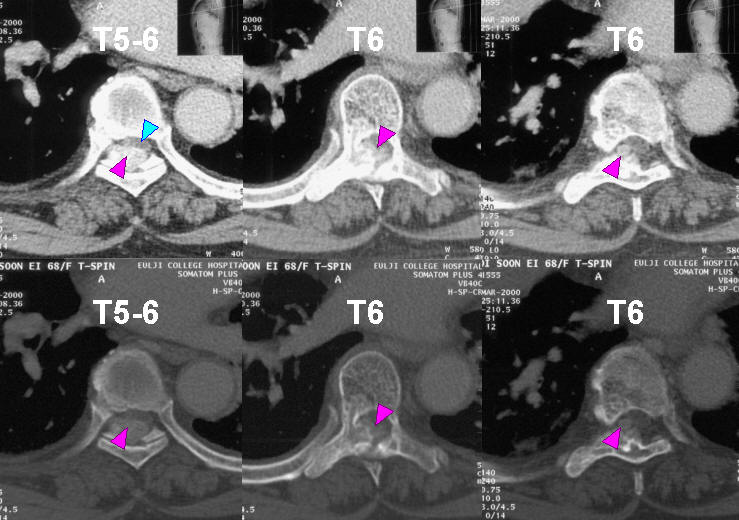
While no abnormal findings were noted on simple roentgenograms, MRI revealed a lesion involving the right posterolateral portion of the vertebral body, the right pedicle, and the whole posterior elements of T6. The lesion invaded into the spinal canal to compress the spinal cord, which was thinned to a crescent-shape. CT scan revealed that the cortical bone was expanded and perforated at the medial portion of the right pedicle.
<Question>
What is the differential diagnosis and treatment?
<Answer>
|
|
|
|



